Johns Hopkins Early Bioterrorism Scenarios
Tracing the origins of "biosecurity"
Introduction
By now it is well known that “Covid-19” was preceded by two decades of planning exercises around “pandemic preparedness,” which are more accurately described as war games (Kennedy Jr., 2021, p. 382; Hughes, 2024, pp. 227-228).
Less well appreciated is the pivotal role of a group of scholars at the Johns Hopkins Bloomberg School of Public Health in getting those exercises off the ground, not as “pandemic preparedness” exercises, but as fictional bioterrorism scenarios. Dark Winter (2001) has achieved notoriety in that regard, but it was preceded by two fictional scenarios involving smallpox and anthrax in 1999, as well as a tabletop exercise called TOPOFF in 2000.
This article addresses those various outputs from 1999 to 2001 with a view to highlighting the origins of “biosecurity” in the “War on Terror” context, as well as the scientific fraud upon which it is premised. Numerous false assumptions embedded in the bioterrorism scenarios from the very beginning have continued to subvert thinking about public health emergencies ever since.
The Johns Hopkins Center for Civilian Biodefense Studies
In 1998, Dean A. Henderson founded the Center for Civilian Biodefense Studies within the Johns Hopkins Bloomberg School of Public Health, ostensibly to increase awareness of the threats posed by biological weapons such as smallpox and anthrax, which terrorists could unleash upon a population, and to develop policy accordingly (Rienzi, 2001).
Henderson is credited, rightly or wrongly, with having led the programme that culminated in the WHO declaring smallpox eradicated in 1980. The end of routine smallpox vaccination, he claimed, created a new vulnerability should smallpox be unleashed in a biological weapons attack for which public health systems were ill prepared.
In 1999, the Center for Civilian Biodefense Studies published two fictional scenarios relating to smallpox and anthrax attacks in the United States, which were ostensibly “intended to provoke thought and dialogue that might illuminate the uncertainties and challenges of bioterrorism” (O’Toole, 1999; Inglesby, 1999).
One of the authors of those scenarios, Tara O’Toole went on to serve as Under Secretary for Science and Technology at the Department of Homeland Security (2009–2013) and as Executive Vice President of In-Q-Tel (the CIA’s venture capital arm) in 2014. The other author, Thomas Inglesby, played a prominent role in Event 201, which forecast a global coronavirus outbreak just weeks before the “novel coronavirus” was announced in late 2019.
In retrospect, the two scenarios appear almost cartoon-like in their overblown descriptions of escalating disaster. Since the two are structurally similar in terms of a US city being overwhelmed by a deadly infectious disease whose spread cannot be contained, we only need to consider one of them to get the gist.
Smallpox: An Attack Scenario
The smallpox scenario involves a bioterrorist attack during a vice-presidential visit to a fictional city with a population of 2.5 million (O’Toole, 1999). The attack takes place on April Fool’s Day, a day seemingly beloved of intelligence agencies when trying to communicate to those in the know that a hoax is taking place (Hughes, 2025).
“Only a terrorist supported by the resources of a rogue state would be able to procure and deploy smallpox,” O’Toole (1999) begins, thus providing a theoretical pretext for an attack on the “rogue state.” As with the Project For A New American Century (2000) and its anticipation of a “catastrophic and catalyzing event – like a ‘new Pearl Harbour,’” the seeds of a cataclysmic state-sponsored terrorist attack against the United States were being sown before “9/11.”
O’Toole’s (1999) smallpox attack scenario proves to be highly unrealistic. It is premised on a raft of assumptions that bear little to no relation to the actual history of smallpox or what is known about it scientifically. Given that the infecting strain of smallpox in the scenario is not bioengineered (i.e., is no different from what has been witnessed historically), there is no reasonable excuse for this failure from a supposed expert in public health.
Far more likely, following Kennedy Jr.’s (2021, p. 382) description of O’Toole as a “CIA spook,” is that we are looking at the infiltration of academia by US intelligence to help create an imaginary threat that could potentially be used for political purposes, such as deciding to invade another country.
Contagion
The fundamental premise of O’Toole’s (1999) scenario is that smallpox has been successfully weaponised and deployed by terrorists.
Yet, there is no evidence that weaponised smallpox has ever existed or could exist (Billauer, 2017, p. 365). For it to be weaponised effectively, it must spread through the air, which is rare at best, despite some reports of it happening in hospital and laboratory settings, where the risk can be reduced (CDC, 2024). Historically, airborne transmission is said to have played a role in only one known smallpox outbreak (in Meschede, Germany, in 1970), yet there are many reasons for doubt (Billauer, 2017, pp. 389-90). In fact, the mode of smallpox transmission has never been conclusively established (Milton, 2012).
Patients in O’Toole’s (1999) scenario start presenting with symptoms 11 days after the attack but are sent away with ibuprofen and told to drink fluids. Smallpox is first confirmed on Day 15 and a contagious disease emergency is declared by the hospital epidemiologist.
This implies that smallpox was spread by patients without obvious symptoms for the first ten days. Yet, according to the CDC (2024), smallpox patients are considered infectious “from the time the first sores appear in the mouth or throat” and smallpox historically was “spread by direct and fairly prolonged face-to-face contact between people.” How exactly, therefore, was the smallpox in the scenario supposed to have spread?
One is reminded of the claim in 2020 that “asymptomatic transmission” drove the “Covid-19 pandemic,” whereby a deadly disease was purportedly spread by outwardly healthy people. There is something obviously fictional about such claims.
The delay in diagnosis in the scenario is painted ominously, as though smallpox has had ample time to spread unchecked. Historically, however, smallpox was commonly not diagnosed for over two weeks, and in some cases over four weeks, yet this never led to a runaway epidemic (Wehrle et al., 1970, p. 676). Today, laboratory testing happens faster than in the past, so there is even less cause for concern.
Second, third, and fourth generation smallpox cases are witnessed in the scenario, with the contagion appearing to spread at roughly the same rate from generation to generation. Yet, in real life smallpox epidemics over the course of the last century, the peak replication rate was typically reached during the first (or perhaps second) generation, then sharply declined (Billauer, 2017, p. 399).
By the end of the scenario two and a half months later, 15,000 cases of smallpox have been reported in 20 US states, resulting in over 2,000 deaths (including a secret service agent and members of the vice-president’s staff, to grab political attention). There are smallpox cases in four other countries (including England, Japan, and Canada).
Yet, it is never quite clear how exactly the disease has spread; in one instance where it appears in a large city in another state, “there was no discernible contact with known smallpox patients or their contacts.” The disease thus has a kind of magical quality that allows it to appear menacingly at any place, any time.
The number of new smallpox cases reported worldwide finally subsides owing to vaccination and the seasonal decrease in the spread of virus as warmer weather returns. Smallpox becomes endemic again.
This seems like a deus ex machina, however, given the inadequate supply of vaccines in the scenario (see below) and the seemingly unstoppable way the disease spreads. It is reminiscent of how Omicron was the latest threatening variant in December 2021, only for “Covid-19” to disappear from the top of the news headlines a few weeks later. In neither case did the end of the crisis seem very convincing.
Fear
Although history and epidemiology suggest there would be no need to panic, fear spreads rapidly in O’Toole’s (1999) smallpox scenario. This largely has to do with media speculation and misinformation.
For example, local and national news networks gather outside the hospital which is sealed off by police following the first confirmed infection. Rumours begin to circulate about what the contagious disease might be. Senior officials from the mayor and the governor all the way up to the FBI director and the President go on television to manage public perception of the event.
As more and more smallpox cases are identified across the city and in an adjoining state, media reports claim that the government does not know how widespread the outbreak might be. The CDC puts all state health departments on alert for possible smallpox.
False reports of an additional attack involving Ebola cause chaos and confusion. Senior officials demand to know why they were not informed about it. Healthcare workers walk off the job. Patients start flooding emergency rooms and doctors’ offices requesting vaccination and evaluation of symptoms.
The irony of all this is that O’Toole’s (1999) scenario is itself a primary driver of fear vis-à-vis a potential smallpox epidemic. Indeed, it was seminal to the creation of a series of bioterrorism simulation exercises orchestrated by O’Toole and her colleagues at Johns Hopkins, all of which were premised on junk science to make a terrifying scenario appear unexpectedly realistic. O’Toole even admitted that she and her colleagues had to “take some of the responsibility” for giving smallpox an extremely scary reputation, although she also blamed the media (cited in Enserink, 2002, p. 1593).
Vaccines
As the smallpox epidemic spreads in the scenario, demand for vaccines dramatically outstrips supply. The assumption is that mass vaccination is the way forward.
This, too, does not match reality. In terms of vaccine supply, it turned out in 2002 that the DoD had 75-90 million doses of smallpox vaccine available, easily enough to deal with a potential outbreak (Billauer, 2017, pp. 408-409). Smallpox vaccine is also effective when diluted, meaning there was enough diluted vaccine for every person in the United States at the time.
As for mass vaccination necessarily being desirable, ring vaccination (i.e., choking off an affected area) means that mass vaccination may not be required, plus not everyone will be susceptible to infection. In general, adequate scientific evidence that mass vaccination is the best mechanism to protect the public “did not (and does not) exist” (Billauer, 2017, pp. 361-362).
In the scenario, with vaccine stocks sufficient to cover only 15% of affected states’ populations, an “accelerated crash vaccine-production program” is announced that will reduce vaccine-manufacturing time to 24 months. That may seem quaint in light of proposals today to reduce the time to 100 days, but it serves as a marker of when this reckless quest to reduce vaccine manufacture time (without concern for long-term safety data) began.
Department of Justice representatives in the scenario raise questions about “potential legal liabilities associated with adverse vaccine effects,” yet vaccination goes ahead regardless. The rush to vaccinate thus looks reckless, much as it did in real life in 2020, although the profits for the vaccine manufacturers will of course be huge – something which is not mentioned by O’Toole (1999).
Non-pharmaceutical Interventions
A city-wide quarantine and travel bans are proposed by the NSC, but are rejected by state authorities. Later in the scenario, there is civil unrest and the National Guard is called in to help police keep order in affected areas. Thus, the scenario consistently tends in the direction of martial law.
Home isolation of unvaccinated contacts is considered in the scenario but disregarded for legal, logistical, and ethical reasons. That “problem” was solved during Covid by using assorted techniques of psychological manipulation to get the public to consent to “self-isolation” and being “locked down.”
In the scenario, the CDC recommends that hospital patients with fever who cannot be definitively diagnosed be quarantined, but hospitals object that they cannot afford to isolate so many patients. The origins of the “overwhelmed hospitals” propaganda that was deployed during Covid can thus be discerned (see Hughes, 2024, pp. 128-134).
In affected areas, tourism, small business, attendance at large public events, and schooling are all severely impacted, as they were during Covid. Domestic and international travel is greatly reduced, with some countries refusing to admit US citizens without proof of recent smallpox vaccination (anticipating the idea of “vaccine passports” in 2020). Other countries impose 14-day quarantines on everyone visiting the country from abroad (anticipating “quarantine hotels” during Covid).
In sum, in O’Toole’s (1999) smallpox attack scenario, we see many of the same outcomes that were witnessed during Covid (e.g., claims about asymptomatic spread being used to drive fear, the push for mass vaccination, travel restrictions, and economic disruption), but they are not grounded in sound science. Rather, the scenario appears motivated by “War on Terror” considerations – two years before the “War on Terror” began.
TOPOFF (May 20-23, 2000)
The little-known TOPOFF exercise of May 2000 has attracted scant attention, perhaps because the main academic journal article on it (co-authored by Dean A. Henderson, Thomas V. Inglesby, Tara O’Toole, and Thomas V. Inglesby, Jr.) is paywalled and does not appear to be freely available online (Henderson et al., 2001).
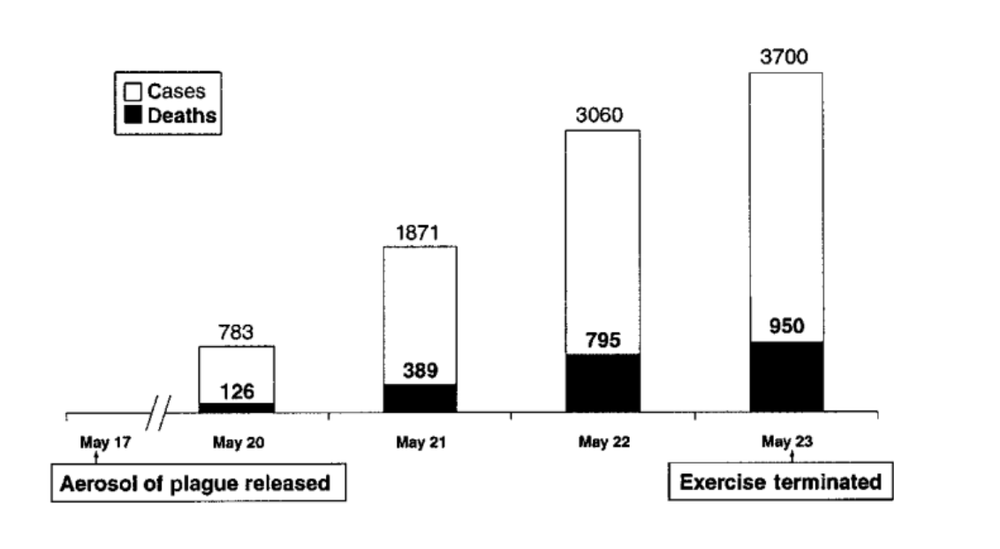
“TOPOFF” is short for “top officials,” and the $3 million exercise simulated how local, state, and federal officials would respond to a chemical weapons event in Portsmouth, NH, a radiological event in the greater Washington, DC area, and a a bioterrorist attack involving the aerosol release of Yersinia pestis (the plague) in Denver, CO. Henderson et al. (2001) deal only with the latter.
The cost and scale of TOPOFF are indicative of government-level planning to deal with a CBRN attack, and it appears to be the first simulation dealing with a bioterrorist attack.
Arguably the most interesting feature of the write-up by Henderson et al. (2001) is the appendix, which notes:
The 1996 Defense Against Weapons of Mass Destruction Act, commonly referred to as the “Nunn-Lugar-Domenici Act,” designates the Department of Defense as “the lead agency to enhance domestic preparedness for responding to and managing the consequences of terrorists’ use of [WMD].” In fiscal year 1997, the Department of Defense received $36 million, whereby it initiated the Domestic Preparedness Program to enhance existing first-responder training in dealing with terrorist incidents involving radiological, nuclear, chemical, and biological weapons [...]. (Henderson et al., 2001, p. 444)
Here we learn that “preparedness” is a military concept and that preparedness programmes were initiated by the Pentagon in 1997.
On March 15, 2000, Colorado House Bill 00-1077 was passed, establishing a 19-person “Emergency Epidemic Response Committee” that would provide expert advice to the governor during an epidemic crisis with legal immunity (Hoffman & Norton, 2000). Hospitals were also granted legal immunity if they followed the executive orders of the governor during such a crisis. The bill also called on healthcare facilities to adopt certain standards for responding to such a crisis (Henderson et al., 2001, p. 444). This real world development is why TOPOFF was set in Colorado.
In the context of an epidemic crisis, TOPOFF highlighted problems in terms of leadership and decision-making, prioritisation and distribution of scarce resources (in particular antibiotics), health care systems becoming overwhelmed, and how to contain the spread of disease (Henderson et al., 2001, p. 436). Similar lessons would allegedly also be applicable to other infectious diseases such as smallpox or pandemic influenza (Hoffman & Norton, 2000).
Contagion
The concept of contagion was critical to TOPOFF, for as one participant reflected,
Many previous bioterrorism exercises dealt with noncontagious diseases. It is just beginning to dawn on us how dramatically different this was as the exercise ended [...] It had all of the [characteristics] of an epidemic out of control” (cited in Henderson et al., 2001, p. 443).
Indeed, only a contagious and deadly disease that threatens to spiral out of control can legitimise the kind of authoritarian measures needed to contain it.
The simulation was guided by “controllers,” who gave the participants “injects” (i.e., new information) at key points. This gave the exercise a heavily pre-scripted feel:
One participant said that it appeared preordained that the plague epidemic would spread beyond local control. Other artificialities of the scenario included a greater risk of person-to-person spread than that which has been reported historically and a laboratory diagnostic process that was tested only on paper. (Henderson et al., 2001, p. 437).
Thus, as with O’Toole’s (1999) smallpox scenario, the “extraordinarily stressful conditions” generated by TOPOFF were based on dubious premises regarding contagion and testing (Henderson et al., 2001, p. 436).
The odds of a disease appearing with this combination of virulence (reports of 3,700 cases with 950 deaths, or over 4,000 cases and over 2,000 deaths) and rapid spread (to other US states, England, and Japan within four days) seem very low based on real world experience.
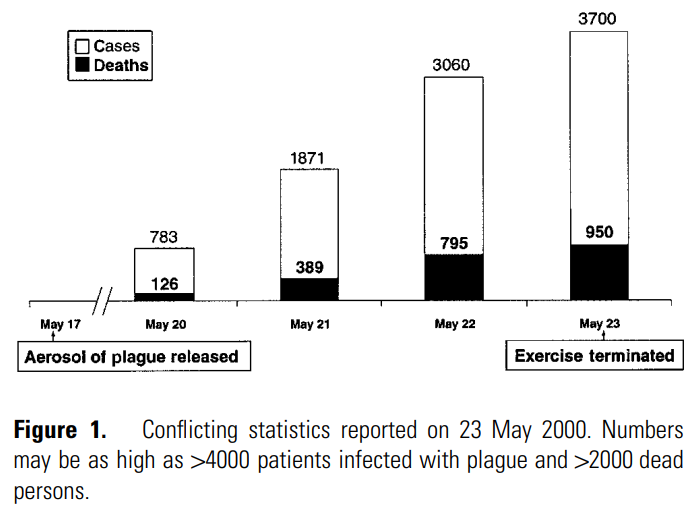
(Source: Henderson et al., 2001, p. 438)
Henderson et al. (2001) do not mention asymptomatic spread, but this is essential to the idea of a highly contagious deadly disease, for otherwise the disease quickly kills the host and thereby reduces the spread. Asymptomatic spread was a key part of “SARS-Cov-2” propaganda in 2020.
Overwhelmed Hospitals
As with “Covid-19” hospital propaganda (Hughes, 2024, pp. 128-134), the hospitals in TOPOFF are quickly overwhelmed and have insufficient antibiotics, ventilators, and beds to deal with a tenfold increase in patients, including the worried well (Henderson et al., 2001, pp. 438, 441). One hospital cannot dispose of dead bodies fast enough which accumulate in the emergency department and wards. The concept of a “security lockdown” at hospitals is discussed but deemed unfeasible. This is the earliest usage of the term “lockdown” that I know of in the “preparedness” context.
One point that is not directly addressed in TOPOFF is “how decision-makers would know a hospital had been overwhelmed, given the absence of historical precedence or systems to make such a judgment” (Henderson et al., 2001, p. 441). Again, we are dealing with fiction and hypotheticals here – or, in the case of “Covid-19,” propaganda.
It is because pneumonic plague patients cannot be isolated that the stay at home order for the general population is issued (Hoffman & Norton, 2000). Thus, we see that population-wide stay at home orders rely on the narrative that hospitals are being overwhelmed. During “Covid-19,” that narrative was demonstrably a lie (Hughes, 2024, pp. 128-134).
Decision Making
It was not clear in TOPOFF who was in charge as participants looked to the state public health agency, the State Attorney General’s office, and federal law enforcement for leadership (Henderson et al., 2001, pp. 438-439). They lamented the diffusion of responsibility, lengthy inefficient conference calls that led to indecision, and the inability of different emergency operations centers to coordinate management and make effective decisions.
The anti-democratic nature of the exercise emerges at this point. One participant commented that “in public health, most decision-making is through democratic processes and consensus building, but for some decisions, this cannot work” (cited in Henderson et al., 2001, p. 439). In a state of emergency, the logic goes, public health must be subordinated to centralised command and control, as we saw during Covid (Corbett, 2021). Planning how that will work is the whole point of “preparedness” exercises.
In an interesting twist, because the Colorado governor did not participate in the simulation, his Emergency Epidemic Response Committee ended up de facto making decisions, even though it did not have the legal authority to do so (Henderson et al., 2001, pp. 439). This is an early precursor of decision-making being outsourced (or being seen to be outsourced) to “experts” during Covid.
Controlling the Spread of Disease
For two of the participants, the “single most important lesson” learned from TOPOFF was that demand for healthcare services would not diminish unless the spread of the disease was controlled (Hoffman & Norton, 2000). The important point here is that the concept of a highly contagious deadly disease has universal, rather than merely local (e.g., city-level) application. It ultimately demands a “global health” infrastructure capable of implementing authoritarian measures at the flick of a switch – as the planners surely knew.
The measures enacted in TOPOFF included travel bans, stay at home orders for the healthy, and the wearing of face masks (“dust masks”), all of which were later features of the response to “Covid-19.” Moreover, the public was told that contagion can only happen “if you are within 6 feet of someone who is infected and coughing” (Henderson et al., 2001, p. 438). Here we see the origin of the antihuman “social distancing” measures in 2020. It is striking that such politically and scientifically dubious measures were an immediate feature of “preparedness” exercises – and were never questioned.
The stay at home order in TOPOFF was particularly problematic. As one observer noted, “They told one million people to stay in their homes. How would we have enforced this?” (cited in Henderson et al., 2001, p. 442). The police and National Guard admitted that they would have been unable to enforce it. Messaging and use of the media therefore became vitally important. One suggestion was “announcing to the public that this was like ‘The 1918 influenza epidemic’” (Henderson et al., 2001, p. 442), a lie that was actually used in 2020 (Hughes, 2024, pp. 120-122).
The planners of TOPOFF understood that messaging would determine the degree to which panicked people might not seek the care they needed or, alternatively, might dangerously crowd health care facilities (Henderson et al., 2001, p. 442). During Covid, messaging such as “STAY HOME. SAVE LIVES. PROTECT THE NHS” saw hospitals under-utilised while patient waiting lists and deaths at home dramatically increased (Hughes, 2024, pp. 129-132).
Closing state borders, though enacted in TOPOFF, was deemed “delusional” by observers, because of disruption to food and essential supplies; notional riots broke out in the exercise.
So-called “holding tanks” were proposed (but not implemented), which would involve quarantining healthy people for seven days before allowing them to leave the state (Henderson et al., 2001, p. 442). “Quarantine hotels” performed a similar function during Covid, only for people entering the country rather than leaving (Nickson & Mullens-Burgess, 2021).
Instead of vaccines, the emphasis in TOPOFF is on antibiotics that can be used to prevent or treat plague. These are in short supply, and difficult decisions have to be made regarding who should be prioritised to receive antibiotics. Logistical and security problems also present themselves in terms of how the antibiotics should be delivered safely from a national stockpile. Only 140 people an hour can be given antibiotic prophylaxis at a centre established for that purpose – nowhere near enough for a city of 1 million (Henderson et al., 2001, p. 440). This is a far cry from “Covid-19,” by which time the problem of how to “vaccinate” the entire world had miraculously been solved.
Contact-tracing was not part of TOPOFF, but was deemed critical in a “real epidemic” (Henderson et al., 2001, p. 442). It was introduced in 2020 to condition the public to accept surveillance right down to the bodily level, albeit in the context of a “pseudopandemic” (Davis, 2021).
Recommendations
TOPOFF concludes that better systems and resources must be put in place in order to manage an attack of the kind simulated. In particular, there needs to be “strong and clear leadership,” “efficient decision-making,” and the “sustained counsel of a multidisciplinary body of experts” (Henderson et al., 2001, p. 443).
Despite a nod to “civil liberties,” the fictitious scenario, premised on dubious science, thereby tends towards technocracy. Real-time surveillance, antidemocratic rule by “experts,” command and control of the population, and major restrictions on personal freedoms amount to a form of authoritarianism instigated in the name of public health.
Of course, the idea is that such measures would only be temporary, until the emergency has passed, but as Agamben (2005) realised, the state of exception created by the “War on Terror” is effectively permanent: democracy and the rule of law can be overridden any time. That is exactly what we have seen in 21st century “emergency” responses to terrorism, financial crisis, the “pandemic,” etc.
Dark Winter (June 22-23, 2001)
In February 2001, the US Commission on National Security/21st Century (the Hart-Rudman Commission) predicted a direct terrorist attack on US soil and recommended the creation of a new homeland security agency.
In June 2001, the Johns Hopkins Center for Civilian Biodefense Strategies (founded in 1998), the Center for Strategic and International Studies, the Analytic Services Institute for Homeland Security (established in April 2001), and the Oklahoma National Memorial Institute for the Prevention of Terrorism (founded in April 2000) collaborated on the Dark Winter exercise that simulated a covert smallpox attack on the United States in early December 2002 – “the first such exercise of its kind” (O’Toole et al., 2002, p. 972). The event took place at Andrews Air Force base just outside Washington, D.C., highlighting its military character.
The ostensible purpose of Dark Winter was to “increase awareness of the scope and character of the threat posed by biological weapons among senior national security experts and to bring about actions that would improve prevention and response strategies” (O’Toole et al., 2002, p. 972). The simulation involved three National Security Council (NSC) meetings held over 13 days.
The exercise took its name from Robert Kadlec’s claim that “it could be a very dark winter for America” on account of lack of smallpox vaccines. Kadlec had also been warning of an imminent anthrax attack since the 1993 World Trade Centre attack and was part of a team of UN weapons inspectors that searched in vain for Saddam Hussein’s suspected stores of anthrax and botulism following the Gulf War (Kennedy Jr., 2021, p. 380).
Key Actors
The “principal designers, authors, and controllers of the Dark Winter exercise” were Tara O’Toole and Thomas Inglesby (Johns Hopkins) and Randy Larsen and Mark DeMier (ANSER) (O’Toole et al., 2002, p. 972). O’Toole and Inglesby were also behind the 1999 smallpox and anthrax scenarios (O’Toole, 1999; Inglesby, 1999), as well as TOPOFF.
The key players in the simulation (and the characters they were playing) included: Sam Nunn (President), James Woolsey (CIA Director), Frank Wisner (Secretary of State), Frank Keating (Governor of Oklahoma), Margaret Hamburg (Secretary of Health & Human Services), David Gergen (National Security Advisor), George Terwilliger (Attorney General), John White (Secretary of Defence), Jerome Hauer (Director, FEMA), John Tilelli (Chairman, JCS), William Sessions (Director, FBI), and Paul Hanely (White House Communications Director).
Of those participants, former Senator Sam Nunn, who played the President, was responsible for the 1996 “Nunn-Lugar-Domenici Act” which placed “preparedness” against terrorist use of WMD in the hands of the Department of Defense. In early 2001, he co-founded the Nuclear Threat Initiative with Ted Turner. Its ethos, like that of “preparedness” exercises, is planning radical measures to deal with a potentially catastrophic but highly unlikely event.
James Woolsey directed the CIA between 1993 and 1995. His involvement in the exercise, alongside that of Tara O’Toole, Randy Larsen and Ruth David, confirms for Robert F. Kennedy Jr. (2021, p. 35) “the intelligence community’s ubiquitous but shadowy presence in biosecurity and all things vaccine.”
In addition, five senior journalists were invited to participate in a mock press conference, namely NBC’s Jim Miklaszewski, CBS’s Mary Walsh, the BBC’s Sian Edwards (who the following year was assistant producer on the fictional documentary Smallpox 2002: Silent Weapon), freelance Lester Reingold, and the New York Times’ Judith Miller (more on her below).
Links to “9/11”
There are multiple linkages between Dark Winter and “9/11” (which took place three months later), making it highly likely that US military intelligence was behind both the “preparedness” exercises and the actual attacks.
For example, the involvement of the Oklahoma National Memorial Institute for the Prevention of Terrorism in Dark Winter is significant, because clear lines of continuity can be traced from the Oklahoma City bombing of 1995 and the attacks of September 11, 2001, including the drafting of the USA Patriot Act and the undermining of the 1878 Posse Comitatus Act (Hughes, 2024, pp. 8-9).
Sam Nunn told Congress a month after Dark Winter that the Soviet Nuclear Threat Reduction Act passed in 1991 (also known as the Nunn-Lugar legislation) involved “some waivers of the posse comitatus statutes” and “needs updating” (cited in Subcommittee on National Security, Veterans Affairs, and International Relations, 2001). Militarising the domestic environment was thus a common concern.
In Dark Winter, 3,000 people were infected with the smallpox virus in three simultaneous attacks on shopping malls in Oklahoma City, Philadelphia, and Atlanta (O’Toole et al., 2002, p. 974). In real life, 11 weeks later, 3,000 people were killed in four simultaneous attacks allegedly involving hijacked aircraft.
In Dark Winter, the intelligence community deems, explicitly without good evidence, that Iraq was behind the biological attack and “Polls of US citizens show overwhelming support for retribution when the attacker is identified” (O’Toole et al., 2002, p. 979). This, of course, is exactly what happened following the September 11 attacks.
In Dark Winter, a fictional news anchor claims that “Iraq might have provided the technology behind the attacks to terrorist groups based in Afghanistan.” Dark Winter participant Judith Miller’s dubious reporting about Iraqi development of WMD for the New York Times (from which the paper later sought to distance itself) was seized upon by the Bush administration to legitimise the US invasion.
Anthrax Attacks
In Dark Winter, an anonymous letter sent to major news agencies demands the immediate removal of all US forces from Saudi Arabia and all warships from the Persian Gulf, lest there be new attacks involving anthrax and plague (O’Toole et al., 2002, p. 979).
In real life, in the weeks following the September 11 attacks (between September 18, 2001, and October 12, 2001), anonymous letters containing lethal anthrax spores were mailed to major news media offices and two U.S. Senators, resulting in 17 infections and five deaths. The Johns Hopkins report on Dark Winter notes this coincidence but finds it strangely unremarkable (O’Toole et al., 2002, pp. 982-3).
Dark Winter participant James Woolsey was tasked by Paul Wolfowitz, a key architect of the Iraq War, with investigating Iraqi involvement in the September 11 attacks and anthrax outbreaks (Harnden, 2001). He sought tirelessly, even under oath (Pringle 2005), to persuade the public of those non-existent links.
Dark Winter participant Jerome Hauer was the managing director of Kroll Inc., informally known as the “CIA of Wall Street,” which managed security at the World Trade Centre. Absent from his WTC office on September 11, 2001, he advised Vice President Cheney’s staff that very evening (i.e. before the anthrax attacks) to take the Ciprofloxacin to prevent anthrax infection (Webb, 2020).
Richard Betts (1998, p. 32), who had ties to the CIA, cited a 1993 study by the US Office of Technology Assessment, claiming that “a single airplane delivering 100 kilograms of anthrax spores [...] by aerosol on a clear, calm night over the Washington, DC, area could kill between one million and three million people.” The idea that “such an attack will take place sooner or later” was reiterated by Lipschutz (1999, p. 412). The anthrax threat was thus manufactured several years before the actual attacks.
In a book-length examination of the anthrax attacks, the late Graeme Macqueen (2014) concludes that “insiders deep within the US state apparatus” were responsible for them, and that these were “the same people who planned the 9/11 attacks.” Given the evidence presented above, it seems hard to disagree.
The anthrax attacks were, in Macqueen’s (2014) view, designed to “facilitate a seizure of power by the executive branch of government through intimidation of Congress and US civil society” and thereby to help initiate the “War on Terror.” The two senators targeted, for instance – Patrick Leahy and Tom Daschle – had sought to slow the rush to war, and the USA PATRIOT Act was passed on October 26, 2001.
Judith Miller, in contrast, was sent harmless white powder
Scientific Fraud
Dark Winter embodies all the same faulty scientific assumptions as O’Toole’s (1999) smallpox attack scenario. Given the obvious political motivation behind the exercise, those faulty assumptions – which no serious public health expert should make – may be regarded as scientific fraud. They can be summarised as follows:
(1) because modern doctors are unfamiliar with smallpox, diagnosis would be delayed, allowing missed cases to infect others; (2) today’s population is largely unvaccinated and therefore more susceptible to infection; (3) increased air travel will disseminate smallpox faster, making tracing difficult; (4) smallpox is highly infective, more so than common diseases such as flu and measles; (5) airborne transmission is a viable means of infecting large populations with a viral disease; (6) there will be at least four generations of spread; (7) the replication rate will be ten to twenty throughout the four generations of spread; (8) the case fatality rate will be thirty percent; (9) there will be an insufficient supply of vaccine for mass vaccination, the preferred means of response, leading to mass hysteria; and (10) it will take three or more weeks to get enough vaccine. (Billauer, 2017, pp. 376-377)
Some of these have already been dealt with in the Smallpox Attack Scenario discussed above, but some additional remarks are worth making.
For example, it is not true that today’s unvaccinated population is more susceptible to smallpox than in the past. To contract smallpox, there must be enough exposure to reach the threshold dose; brief contact usually fails to induce illness, so much so that variolation was once used to prevent the disease (Billauer, 2017, p. 401).
Far from international air travel increasing the likelihood of a pandemic, the number of disease outbreaks has decreased while air travel has greatly increased (Billauer, 2017, p. 404). This probably has to do with increased host resistance owing to modern industrialized life-styles involving better hygiene, medical care, intervention and nutrition (Roberts, 2003, p. 660).
Smallpox is far less infectious than measles and various strains of flu; according to Enserink (2002, p. 1592), it is “a barely contagious and very slow-spreading infection.”
Not only is airborne transmission of smallpox dubious for reasons given above, but Dark Winter falsely assumes that the winter weather in Oklahoma City in December 2002 will increase the spread of the virus. In reality, there was an ice and snow storm in Oklahoma City in early December 2002, meaning that people would mostly have stayed at home rather than going out and spreading the virus (Billauer, 2017, p. 372).
As in O’Toole’s (1999) smallpox scenario, the smallpox epidemic in Dark Winter lasts three to four generations, with 3,000 people infected in the first generation and 3,000,000 by the fourth, implying a roughly constant replication rate across all four generations (Billauer, 2017, p. 365). This is nonsense for the reasons given above.
Dark Winter assumes a replication rate of at least ten for smallpox, which, according to biological weapons specialist Milton Leitenberg, is over three times the historical average (cited in Bain & Cirincione, 2006). According to a team led by the CDC’s Martin Meltzer, a replication rate of two is more representative of actual past epidemics (see Enserink, 2002, p. 1593).
Dark Winter envisages “up to three million cases and one million deaths from smallpox,” implying a case fatality rate (CFR) of 33% (O’Toole et al., 2002, p. 975). Yet, the worst-case CFR for smallpox over the last century is between 15%-20% and for post-WWII non-endemic countries falls to 16% or lower (Billauer, 2017, p. 403).
In Dark Winter, 12 million vaccine doses are available at the time of the outbreak and new vaccine doses will not be available for at least four weeks. Vaccine scarcity induces panic and hysteria in the exercise. Yet, in reality, the CDC had 15 million vaccine doses on hand in December 2002, the DoD had a further 75-90 million doses, and Anthony Fauci determined that vaccine dilution was effective at 1:10, implying more than enough vaccine for the entire US population (Billauer, 2017, p. 366).
In sum, far from being informed by scientific expertise, Dark Winter proves to be nothing more than “an imaginary fable” bearing no discernible relation to reality (Billauer, 2017, p. 364).
The Attack on Civil Liberties
The scientific fraud in Dark Winter is far from innocent, because it is used to legitimise the most draconian of measures in response to the notional bioterrorism attack.
For example, the push towards martial law in Dark Winter is undeniable. One slide from the original presentation moots “forcible restrictions on citizens” and the “need for martial law.”
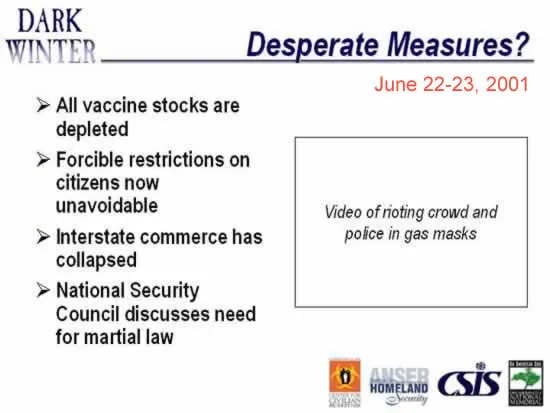
(Source: Democracy Manifest, 2024, with event date added)
Underscoring the need for authoritarian measures, O’Toole et al. (2002, p. 978) ask:
Should patients with smallpox be confined to facilities dedicated to care for them? Should contacts of patients be forced to remain at home or in dedicated facilities until they are proven to be free of smallpox? Should national travel restrictions be imposed? How can disease containment best be balanced against economic disruption and the protection of civil liberties? To what extent can and should the government infringe upon civil liberties? Under what conditions can those powers be exercised?
This is brazen. A key purpose of the exercise was evidently to explore how far the government could go in infringing upon civil liberties under the pretext of a bioterrorism attack. Again, this was three months before “9/11,” suggesting that planning for using terrorist attacks to undermine civil liberties was already at an advanced stage.
Vaccines
With only 12 million doses available in Dark Winter, how should vaccines best be distributed? Should vaccination be made mandatory? (O’Toole et al., 2002, p. 977). Here, the gruesome spectre of mandatory vaccination, which violates the Nuremberg Code, is raised, even though the scientific foundation of the exercise is bogus.
As vaccine supplies dwindle in the exercise, public unrest grows and misinformation about the smallpox outbreak starts to appear. In words that anticipate the Covid “lockdowns” almost two decades later, “Schools are closed nationwide. Public gatherings are limited in affected states. Some states limit travel and nonessential gatherings” (O’Toole et al., 2002, p. 977). There is mandatory isolation of those infected as well as their contacts. Again, all these draconian measures are based on scientific fraud.
Finding themselves in a so-called “war,” which predates the announcement of the “War on Terror,” Dark Winter participants opt for “a crash production program for new smallpox vaccine, despite unresolved liability issues,” and accept the offer of a Russian smallpox vaccine (O’Toole et al., 2002, p. 979). Thus, rapid vaccine production (which ignores liability issues and the usual FDA regulations) and international collaboration were proposed as the way out, just as they were during Covid.
Dark Winter participants “worried that it would not be possible to forcibly impose vaccination or travel restrictions on large groups of the population without their general cooperation” (O’Toole et al., 2002, p. 982). Sam Nunn, for instance, observed that “The federal government has to have the cooperation from the American people. There is no federal force out there that can require 300,000,000 people to take steps they don’t want to take.”
The problem remaining was, thus, how to get the population to consent to its own oppression, and the answer was largely supplied in 2020.
The Congressional Hearings of July 23, 2001
One month after Dark Winter, on July 23, 2001, two Congressional hearings were held on the theme of bioterrorism. Common to both was the need to give the Federal Emergency Management Agency (FEMA) a central coordinating role in responding to bioterrorism attacks.
The Subcommittee on National Security, Veterans Affairs, and International Relations (2001) conducted a hearing titled “Combatting Terrorism: Federal Response to a Biological Weapons Attack.” Meanwhile, the International Security, Proliferation and Federal Services Subcommittee (2001) conducted a hearing titled “FEMA’s role in managing bioterrorist attacks and the impact of public health concerns on bioterrorism preparedness.”
Those addressing the first hearing included John Hamre (President and CEO of the Center for Strategic and International Studies), Frank Keating (Governor of Oklahoma), former senator Sam Nunn (Chairman and CEO of the Nuclear Threat Initiative), Margaret Hamburg (Vice President of NTI Biological Programs), Jerome Hauer (Managing Director, Kroll Associates), Dean Henderson (Director, Johns Hopkins Center for Bioterrorism Prevention), Major General Ronald O. Harrison (Adjutant General of Florida), Major General William A. Cugno, (Adjutant General of Connecticut), Dr. James Hughes and James LeDuc (Directors, National Center for Infectious Diseases, Centers for Disease Control and Prevention), Patricia Quinlisk (medical director and State epidemiologist, Iowa Department of Public Health) and Jeffrey Duchin (Head of Communicable Disease Control, Epidemiology and Immunization, Seattle and King County, WA).
In the first hearing, Nunn told Congress that “FEMA is going to have to play a big role.” Keating proposed that healthcare professionals be “trained at the State level to recognize [...] contagious diseases, and then to be able to access perhaps through FEMA the body of knowledge necessary to respond quickly.” Hauer, who played the role of Director of FEMA in Dark Winter, claimed that “FEMA needs to be the overarching agency that does the coordination of this at the Federal level and then rely on agencies like HHS for [...] expertise.” Hamburg testified that the “comprehensive coordinator” should be FEMA. Cugno advocated for a central role for the Adjutant General, who commands the State Office of Emergency Management in 23 US states and is “keenly aware of the role of FEMA.”
The second hearing was all about “FEMA’s role in managing bioterrorist attacks.” O’Toole told the Subcommittee “I would encourage FEMA, in particular, to design, assess and use drills that might reveal the vulnerabilities and inspire coordination and improve awareness of the issues and options that a biological weapons attack would present to decisionmakers” (cited in International Security, Proliferation and Federal Services Subcommittee, 2001).
Such options, judging by the first hearing, principally involve mass vaccination and forced isolation/quarantine of the population. On mass vaccination, for instance, Hauer observed that “The logistical infrastructure necessary to vaccinate the people of New York City, Los Angeles, Chicago is just – would be mind-boggling.” Hamre noted that “we would have to waive a fair amount of Federal regulation in order to get vaccines available on an expedited basis.” Hamburg asked “what does it mean to in an emergency use drugs or vaccines that haven't yet been licensed?,” noting that in Dark Winter “we made the decision early on that given the gravity of the situation, we would certainly move forward.” The pseudoscience in Dark Winter was thus successful in legitimising the push for injecting the population with unlicensed substances, a dominant feature of the “Covid-19” debacle two decades later.
In terms of forced isolation/quarantine, Hamre testified that in Dark Winter “we were confronting the reality that forcible constraint of citizens' behavior was probably going to be required to be able to stop that fourth generation of infections.” This would mean that “you at gunpoint put your own citizens under, in effect, house arrest.” Hauer asked “At what point in time do we use force on the citizens of this country? And who makes that decision?,” noting that “the use of military assets” would be required.
Thus, within the space of a month, Dark Winter had translated into recommendations to Congress that legal provisions be made for mass vaccination and house arrest, to be enforced by the military under FEMA’s coordination.
The Model State Emergency Health Powers Act
The Model State Emergency Health Powers Act (“the Act”; MSEHPA) was drafted by the Center for Law and the Public's Health (CLPH) at Georgetown and Johns Hopkins Universities at the request of the CDC days after the first cases of anthrax were confirmed on October 4, 2001 (Gostin, 2003, p. 20). Its aim was to provide US states with the necessary powers to detect and contain a potentially catastrophic disease outbreak (Gostin, pp. 4-5).
A first draft was ready by October 23, 2001 and a revised version was published on December 21, 2001 (MSEHPA, 2001).
Some of the language in the original draft was removed from the revised version, such as “Control of Persons” (which became “Protection of Persons”), “mandatory medical examinations” (“medical examination and testing”), “shall be performed immediately upon the order of the public health authority without resort to judicial or quasi-judicial authority” (changed to requiring judicial review) and “to compel a person to be vaccinated and/or treated for an infectious disease” (changed to allow exemptions on religious grounds). Nevertheless, the original intent to “control” people through “mandatory” testing and compulsory vaccination without recourse to judicial authority is clear.
The premise of the Act is that
Emergency health threats, including those caused by bioterrorism and epidemics, require the exercise of extraordinary government functions [...] The Model State Emergency Health Powers Act therefore grants specific emergency powers to state governors and public health authorities. (MSEHPA, 2001, p. 6)
In the case of smallpox, which featured in Dark Winter, we know that premise to be false for the reasons given above.
Nevertheless, based on that premise, a raft of draconian legislation was proposed, particularly in Article VI ( “Special Powers During a State of Public Health Emergency: Protection of Persons”). For example, Section 602(c) provides that
The public health authority may isolate or quarantine, pursuant to Section 604, any person whose refusal of medical examination or testing results in uncertainty regarding whether he or she has been exposed to or is infected with a contagious or possibly contagious disease or otherwise poses a danger to public health.
In other words, anyone suspected of being infected who refuses medical examination can be forcibly isolated/quarantined. The same fate awaits “persons who are unable or unwilling for reasons of health, religion, or conscience to undergo vaccination” in Section 603(a)(3). They may be held in isolation for up to 30 days, and this can be renewed.
One of the authors of the Model State Emergency Health Powers Act addressed some of the many concerns that had made it “a lightning rod for criticism” (Gostin, 2003, p. 5). The revised version, he noted, made clear that it was not intended for endemic diseases such as influenza or HIV/AIDS, that a governor’s decision could immediately be overridden by a majority decision in the legislature, and that any criminal penalties for refusing to comply with public health orders had been removed (Gostin, 2003, p. 21).
Nevertheless, he had no problem with such people being forcibly isolated or quarantined: “the Model Act does not permit public health officials to vaccinate, test, or medically treat people against their will. At most, individuals may be isolated or quarantined to reduce their risk to others” (Gostin, 2003, p. 26).
Such measures, he argued, could be justified by “rethinking the public good” so as to give greater importance to the “well being of the populace” (Gostin, 2003, p. 31). Here we see a precursor of the “common good” rhetoric witnessed during Covid. In an emergency, we are told, individual rights and liberties must be subordinated to “the common good.”
But how do we know it is a genuine emergency? Gostin’s (2003) entire defence of the MSEHPA rests on a bioterrorism threat assessment cooked up by the intelligence agencies. For example,
A report by the National Intelligence Council for the Central Intelligence Agency concluded that infectious disease is not only a public health issue, but also a problem of national security: the U.S. population is vulnerable to bioterrorism as well as emerging and reemerging infectious diseases. (Gostin, 2003, p. 7)
Or again: “In 1999, the U.S. Commission on National Security in the 21st Century concluded that biological agents are the most likely choice of weapons for disaffected states and groups” (Gostin, 2003, p. 8). And “Documents recovered in Afghanistan suggest that Al Qaeda has conducted extensive research on weapons that can cause mass fatalities, including biological weapons” (Gostin, 2003, p. 9). He also cites TOPOFF and Dark Winter, which were products of the national security state.
Gostin (2003) does not realise that those exercises are premised on highly implausible scientific assumptions. Instead, he emphasises that, under Article IV of the Act, “a Governor may declare a public health emergency only if a series of demanding threshold conditions are met,” including “a high probability of a large number of deaths” and/or disabilities (2003, p. 17). Technically, no one needs to have died; there need only be the “imminent threat of an illness or health condition” (Gostin, 2003, p. 17). Therefore, the legitimacy of the Act depends entirely on whether the threat assessment is credible. Judging by Dark Winter, it clearly is not.
Impacts on Policy, Public Health Discourse, and Education
The work of O’Toole, Inglesby, and Henderson between 1999 and 2001 was clearly aimed at conjuring scare stories aimed at benefiting the military-pharmaceutical complex, and in that respect, it was successful. Their scenarios, though pie-in-the-sky, had real world impact.
For example, following the 2001 anthrax scare, US bioterrorism priority lists were updated as the CDC refined its list of high-profile bioagents based on the conclusions of Henderson and his Working Group on Civilian Biodefense (Billauer, 2017, p. 349). Smallpox featured prominently as the most dangerous of the Class A bioterrorist agents.
The Model State Emergency Health Powers Act went on to serve as “an important catalyst for state action in the field of bioterrorism preparation” (Martin, 2004).
Nunn told Congress in July 2001 that a US public health system capable of dealing with the bioterrorist threat will need “some real money spent” (cited in International Security, Proliferation and Federal Services Subcommittee, 2001). The Project BioShield Act of 2004 authorised $5.6 billion over ten years to accelerate the development and acquisition of medical countermeasures against chemical, biological, radiological, and nuclear (CBRN) threats. By 2017, allocations to US biodefence had reached $80 billion (Billauer, 2017, pp. 355-356). Such massive spending diverts resources from more quotidian public health concerns such as combatting infectious diarrhea, which claims two millions lives a year (Billauer, 2017, p. 413).
O’Toole called for “a substantial research and development program that involves biomedical talent in the private sector and the universities” (cited in International Security, Proliferation and Federal Services Subcommittee, 2001). Federal spending created large incentives for institutions and individuals to produce outputs that aligned with the biodefence agenda, even where this involved twisting the facts and the scientific evidence.
A shift occurred in public health discourse towards uncritical endorsement of vaccines. As Schrader & Campion (2003) put it, “The public health question has changed from ‘Are we at risk from a smallpox attack?’ to ‘Whom should we be vaccinating?’” Their own attitude was “If necessary, we must also roll up our sleeves and be vaccinated” – perfect compliance, generated through a series of scientific fantasies and fairy-tales.
By 2007, the United States operated over 1,350 level three biosafety labs and 15 level four labs, ostensibly to guard against bioterrorist and pandemic threats. Given that those threats appear wildly overstated, and that the results of the research from those labs are “murky at best” (Billauer, 2017, p. 351), we might wonder what else is going on in those labs.
During the 2009 confirmation hearings for O’Toole’s nomination to undersecretary at the Department of Homeland Security, Democratic Senator Carl Levin of Michigan noted that “many top scientists have said that the Dark Winter exercise was based on faulty and exaggerated assumptions about the transmission rate of smallpox” (cited in Kennedy Jr., 2021, p. 386). That did not block O’Toole’s appointment, however, because the exaggerated assumptions are an integral part of “homeland security.”
When it came to “Covid-19,” the Model State Emergency Health Powers Act (including subsequent revisions of it) was invoked by US states. As was feared by critics in the early days, the Act served to legitimise “an unprecedented increase in unilateral lawmaking by governors,” thereby undermining democratic legitimacy (Weiss, 2021, p. 1853). This was despite the fact that the Act was “not intended to apply to chronic emergencies such as COVID-19, with unilateral decisionmaking going on for over a year, or to responses such as social distancing regulations or mass lockdowns” (Weiss, 2021, pp. 1876-1877).
Conclusion
The erstwhile Secretary of Health and Human Services, Donna Shalala, stated at a White House press briefing on January 22, 1999 that “Bioterrorism is perhaps the first time in American history in which the public health system is integrated directly into the national security system” (“Press Briefing,” 1999).
That was precisely the point of the early bioterrorism simulations involving Johns Hopkins scholars between 1999 and 2001, as well as the many “pandemic preparedness” simulations that have taken place since. They essentially propose means of bringing the public healthcare system under the control of the national security state.
The smallpox and anthrax scenarios by O’Toole (1999) and Inglesby (1999), the $3 million TOPOFF exercise, and Dark Winter were all aimed at shifting perception and mainstreaming the credibility of a major bioterrorist attack in the United States, so that new measures could be proposed to deal with the alleged threat. As with the “War on Terror” in general, those measures hand disproportionate power to the executive branch and represent an affront against a free society.
Just as it is scientifically impossible that two planes caused three skyscrapers to disappear on September 11, 2001, so the Johns Hopkins bioterrorism scenarios are laced with scientific fraud. Virtually all of their key assumptions, certainly about smallpox, are flawed. Given that Dark Winter predicts with a high degree of precision what would later unfold following the “9/11” attacks, there is almost no chance that the authors of those scenarios simply “got it wrong.”
Rather, they were actively helping to bring about a new reality in which the public felt ever-threatened by the possibility of terrorist attacks involving WMD and was willing to cede its liberties accordingly. As Billauer (2017, p. 347) puts it, “rather than modeling actual weapons of mass destruction, in essence, the exercise [Dark Winter] artificially creates weapons of mass hysteria.”
This set a precedent that has continued up to the present day, whereby threat projections for bioterrorism and pandemic planning have consistently used mathematical modelling to come up with “reasonable worst scenarios” while ignoring biological plausibility, relevant historical data, and modern medical practice. Thus,
Past pandemic projections for avian flu, smallpox, anthrax, swine flu, and Ebola grotesquely overestimated the disease’s incidence and mortality illustrating deficiencies in current models, and in some cases, generating adverse health consequences more severe than any realistic epidemic. (Billauer, 2017, p. 347)
Exactly the same was true of “Covid-19.” The threat was wildly overhyped (Hughes, 2024, Chap. 4) while the measures instigated to mitigate it proved catastrophic for many people.
A quarter of a century after the US anthrax attacks, which were perpetrated by the deep state (MacQueen, 2014), there has still not been a major bioterrorist attack on a Western country. This gives the lie to decades of fearmongering claims about the inevitability of such an attack given the ease with which it could allegedly be carried out.
In the final analysis, we should see bioterrorism and “pandemic preparedness” planning as fundamentally illegitimate. They are not about protecting the public against deadly diseases, but, rather, devising cunning ways of persuading the public to part with its liberties.
References
Agamben, G. (1998). Homo sacer: Sovereign power and bare life. Stanford University Press.
Agamben, G. (2005). State of exception (Trans. K. Attell). Chicago University Press.
Bain, B., & Cirincione, J. (2006). Exaggerating the threat of bioterrorism. Carnegie Institute for International Peace. https://carnegieendowment.org/research/2006/03/exaggerating-the-threat-of-bioterrorism.
Betts, R. (1998). The new threat of mass destruction. Foreign Affairs, 72(1), 26-41. http://www.columbia.akadns.net/itc/sipa/S6800/courseworks/newThreat.pdf.
Billauer, B.P. (2017). Weapons of mass hysteria, faulty biothreat predictions, and their impact on national (in)security: A case-study of smallpox. Health Matrix, 27(1). https://scholarlycommons.law.case.edu/cgi/viewcontent.cgi?article=1610&context=healthmatrix.
CDC. (2024, October 22). How smallpox spreads. https://www.cdc.gov/smallpox/causes/index.html.
Corbett, K. P. (2021, August 7). The “‘Nazification” of the NHS. The Light Paper. https://thelightpaper.co.uk/assets/pdf/Light-12h.pdf.
Davis, I. (2021). Pseudopandemic. Independently published.
Democracy Manifest (2024, September 8). Quarantines and vaccines… https://democracymanifest.substack.com/p/quarantines-and-vaccines.
Enserink, M. (2002). News focus bioterrorism: How devastating would a smallpox attack really be? Science, 296, 5573. https://doi.org/10.1126/science.296.5573.1592.
Gostin, L.O. (2003). The Model State Emergency Health Powers Act: Public health and civil liberties in a time of terrorism. Health Matrix, 13(1), 3-32, https://scholarlycommons.law.case.edu/cgi/viewcontent.cgi?article=1387&context=healthmatrix,
Harnden, T. (2001, October 26). Building the case against Iraq.” The Telegraph. https://www.telegraph.co.uk/news/worldnews/middleeast/iraq/1360627/Building-the-case-against-Iraq.html.
Henderson, D.A., Inglesby, Jr., T.V., O'Toole, T., & Inglesby, T.V. (2001). A plague on your city: Observations from TOPOFF. Clinical Infectious Diseases, 32(3), 436-445. https://doi.org/10.1086/318513.
Hoffman, R.E., & Norton, J.E. (2000). Lessons learned from a full-scale bioterrorism exercise. Emerging Infectious Diseases, 6(6), 652-653. https://doi.org/10.3201/eid0606.000617.
Hughes, D.A. (2024). “Covid-19,” psychological operations, and the war for technocracy. Palgrave Macmillan.
Hughes, D.A. (2025). Were they mocking us? https://dhughes.substack.com/p/mockery.
Inglesby, T.V. (1999). Anthrax: A Possible Case History. Emerging Infectious Diseases, 5(4). https://wwwnc.cdc.gov/eid/article/5/4/99-0419_article.
International Security, Proliferation and Federal Services Subcommittee. (2001, July 23). FEMA’s role in managing bioterrorist attacks and the impact of public health concerns on bioterrorism preparedness. https://www.govinfo.gov/content/pkg/CHRG-107shrg75441/html/CHRG-107shrg75441.htm.
Kennedy Jr., R.F. (2021). The real Anthony Fauci. Bill Gates, big pharma, and the global war on democracy and public health. Skyhorse.
Lipschutz, R.D. (1999). Terror in the suites: Narratives of fear and the political economy of danger. Global Society, 13(4), 411-439. https://doi.org/10.1080/13600829908443202.
MacQueen, G. (2014). The 2001 anthrax deception. The case for a domestic conspiracy. Clarity Press.
Martin, W. (2004). Legal and public policy responses of states to bioterrorism. American Journal of Public Health, 94(7), 1093-1096. https://doi.org/10.2105/AJPH.94.7.1093.
Milton, D.K. (2012). What was the primary mode of smallpox transmission? Implications for biodefense. Frontiers in Cellular & Infection Microbiology, 2(150). https://doi.org/10.3389/fcimb.2012.00150.
Model State Emergency Health Powers Act. (2001, December 21). https://publichealth.jhu.edu/sites/default/files/2023-06/msehpa.pdf.
Nickson, S., & Mullens-Burgess, E. (2021). Hotel quarantine. Institute for Government. https://www.instituteforgovernment.org.uk/article/explainer/hotel-quarantine.
O’Toole, T. (1999). Smallpox: An attack scenario. Emerging Infectious Diseases, 5(4). https://wwwnc.cdc.gov/eid/article/5/4/99-0416_article.
O’Toole, T, Mair, M., & Inglesby, T.V. (2002). Shining light on ‘Dark Winter.’ Clinical Infectious Diseases, 34(7), 972-983. https://doi.org/10.1086/339909.
Press briefing by Attorney General Janet Reno, Secretary of H.H.S. Donna Shalala, and Richard Clarke, President's National Coordinator for Security, Infrastructure and Counterterrorism. (1999, January 22). The American Presidency Project. https://www.presidency.ucsb.edu/documents/press-briefing-attorney-general-janet-reno-secretary-hhs-donna-shalala-and-richard-clarke.
Pringle, E. (2005, November 16). Bush gang swore Saddam was behind 9/11 in lawsuit. Counterpunch. https://www.counterpunch.org/2005/11/16/bush-gang-swore-saddam-was-behind-9-11-in-lawsuit/.
Project for a New American Century. (2000, September). Rebuilding America’s defences. https://resistir.info/livros/rebuilding_americas_defenses.pdf.
Rienzi, G. (2001). Bioterrorism puts center in headlines. The Gazette Online. https://pages.jh.edu/gazette/2001/05nov01/05center.html.
Roberts, I. (2003). Biological warfare and the people of Iraq, International Journal of Epidemiology, 32(4), 660-661. https://doi.org/10.1093/ije/dyg226.
Schrader, T.L., & Campion, E. (2003). Smallpox vaccination – The call to arms. New England Journal of Medicine, 348. https://doi.org/10.1126/science.296.5573.1592.
Subcommittee on National Security, Veterans Affairs, and International Relations. (2001, July 23). Combatting Terrorism: Federal Response to a Biological Weapons Attack. https://www.govinfo.gov/content/pkg/CHRG-107hhrg81593/html/CHRG-107hhrg81593.htm.
Webb, W. (2020, April 1). All roads lead to Dark Winter. The Last American Vagabond. https://www.thelastamericanvagabond.com/all-roads-lead-dark-winter/.
Wehrle, P.F., Posch, J., Richter. K.H., & Henderson, D.A. (1970). An airborne outbreak of smallpox in a German hospital and its significance with respect to other recent outbreaks in Europe. Bulletin of the World Health Organisation, 43(5), 669-79. https://iris.who.int/items/808ac2ce-74c0-434c-ad38-a5dfac9e89b9.
Weiss, A. (2021). Binding the bound: State executive emergency powers and democratic legitimacy in the pandemic. Columbia Law Review, 121(6), 1853–1892. https://columbialawreview.org/content/binding-the-bound-state-executive-emergency-powers-and-democratic-legitimacy-in-the-pandemic/.
Support My Work
If you valued this content and are not a paid subscriber, please consider leaving a one-off tip for an amount of your choosing.
If you would like to make a one-off or recurring donation to help fund my work in general, I would be most grateful. There are numerous ways of doing so, including wire transfer, Paypal, UK cheques, and Buy Me A Coffee.
If you have not done so already, please consider taking out a subscription to davidahughes.net or upgrading an existing one – free, paid, or gold-tier.